Ophthalmology is one of the fastest-growing branches of medicine, with laser vision correction being its most dynamic field. It is a remarkable invention and a true achievement of modern science. I have been specializing in vision correction for 15 years, witnessing and participating in an incredible technological revolution. Today, the scope of knowledge, predictability, and precision in this field is unprecedented.
From these years of practice and the experience of 40,000 procedures, I have learned one vital lesson: precision and diligence are the most valuable assets in this work.
There is no single "best" method
With so many correction methods available, choosing the right one can be difficult for a patient – especially since there is no objectively or universally “best” method for everyone.
Each technique has unique attributes designed to benefit a specific group of patients.
Only science – our work is based on scientific facts
To make it easier to understand how different vision correction methods are applied, we can use the concept of “Effective Reshaping Power” (ERP).
Effective Reshaping Power is the potential of a specific correction method (SMILE, Femtolasik, PRK, EBK) to correct a particular vision defect – essentially, it indicates which method is most effective for a given condition.
For myopia (shortsightedness), the most effective methods (highest ERP) are, in order: SMILE, FemtoLASIK, PRK
For hyperopia (farsightedness): FemtoLASIK, SMILE Hyperopic, PRK
For myopic astigmatism: SMILE, FemtoLASIK, PRK
For hyperopic astigmatism: FemtoLASIK, PRK
For astigmatism: FemtoLASIK, PRK
Precise, More Precise, Most Precise
It is important to note that when considering which method to use, we evaluate not only its effectiveness (the ERP factor) but also the amount of available corneal tissue.
Therefore, in some cases, the choice of method falls not on the one with the highest ERP, but on the one best suited to the specific patient’s situation.
Vision Correction Methods
ReLex Smile
Who is ReLex SMILE for?
Patients with shortsightedness (myopia) up to -10.0 diopters.
Patients with myopic astigmatism up to -5.0 diopters, with an accompanying spherical error up to -10.0 diopters.
Why choose ReLex SMILE?
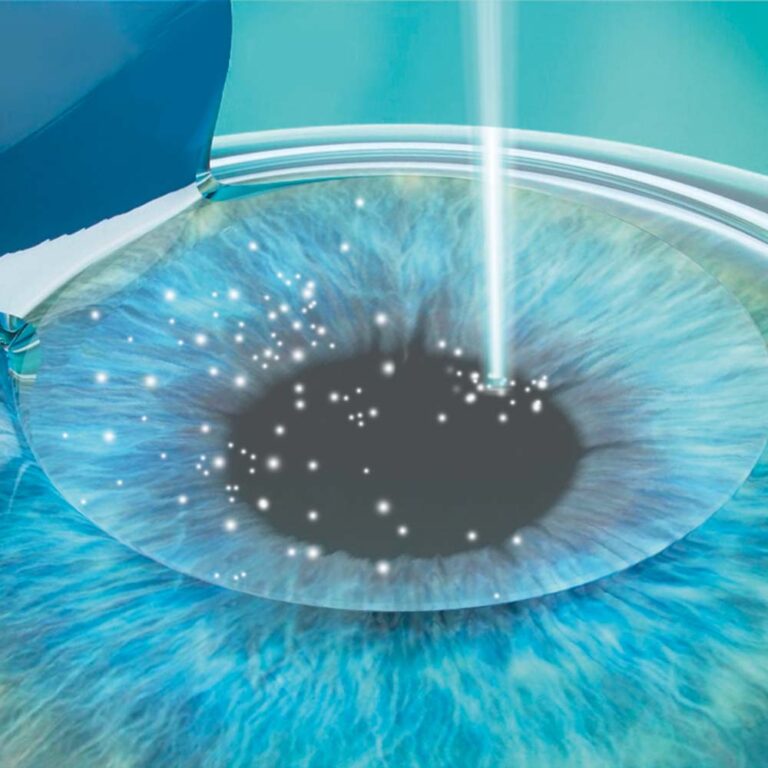
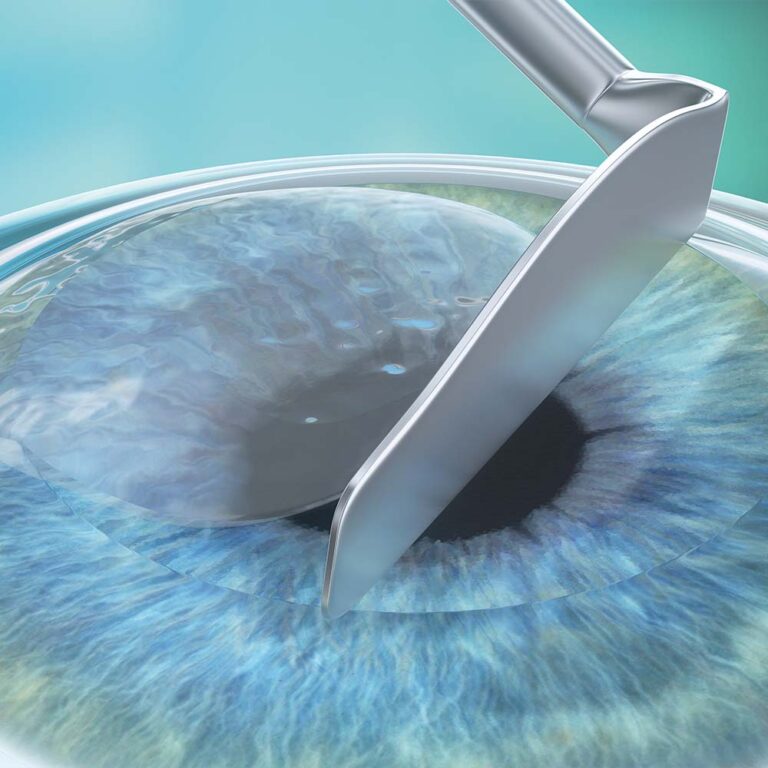
Minimal corneal interference: Uses a micro-incision (microport) only 2.8 millimeters long.
Minimal disruption to the corneal nerve plexus.
Maximum corneal stability and strength following the procedure.
Lowest susceptibility to the effects of potential future eye injuries.
One of the specialized methods for treating selected cases of keratoconus (Aztec protocol).
Shortsightedness (Myopia), High Shortsightedness (High Myopia), Myopic Astigmatism, Presbyopia in Myopia
Patients with farsightedness (hyperopia) up to +6.0 diopters.
Patients with astigmatism up to 6.0 diopters, with an accompanying spherical error up to -10.0 diopters.
Patients with near vision impairment (presbyopia).
The procedure can also be used for shortsightedness (minus errors), although this is less common due to the availability of the SMILE technology alternative.
Why choose FemtoLasik?
High EMO (Effective Modifying Power) coefficient: This method is highly effective for treating vision impairments that are more resistant to correction, such as farsightedness (hyperopia), hyperopic astigmatism, and complex astigmatism.
Easy access for future adjustments: Due to the ease of accessing the treatment zone (laser area), this method is an excellent choice for patients who may require re-correction in the future (those with farsightedness developing after age 40 or presbyopia)
Combined correction protocols: FemtoLasik allows for the simultaneous application of protocols designed to correct both distance and near vision, such as Presbyond and Presbymax.
Patients with shortsightedness (myopia) up to -8.0 diopters.
Patients with farsightedness (hyperopia) up to +4.0 diopters.
Patients with myopic astigmatism up to -2.0 diopters, with an accompanying spherical error up to -10.0 diopters.
Why choose Presbyond?
Technically, Presbyond is identical to the Femto-LASIK method. These techniques differ only in their ablation profile (the ablation profile refers to the laser’s effect on the corneal surface or the specific change in the corneal shape induced by the laser).
The specialized ablation profile used in the Presbyond method provides the patient with additional near-vision power compared to standard monovision.
Presbyond allows for quick and easy access to the ablation zone (the area where the laser treatment is performed) should a re-correction be necessary due to the age-related progression of near-vision impairment.
Patients with shortsightedness (myopia) up to -3.5 diopters, including those with accompanying astigmatism.
Patients with farsightedness (hyperopia) up to +2.5 diopters.
Patients with astigmatism up to ±2.5 diopters
Why choose EBK?
EBK is a surface procedure where the corneal epithelium is removed mechanically—without the use of alcohol.
The absence of alcohol in this method ensures a faster regrowth of the corneal epithelium, making the post-operative recovery period significantly milder and more comfortable.
Since there is no need to create a corneal flap, EBK is an excellent option for patients with thin corneas
Mild Shortsightedness (Mild Myopia) and Myopic Astigmatism, Mild Farsightedness (Mild Hyperopia) and Hyperopic Astigmatism, Mild Astigmatism
Patients with shortsightedness (myopia) up to -3.5 diopters, possibly with accompanying astigmatism.
Patients with farsightedness (hyperopia) up to +2.5 diopters.
Patients with astigmatism up to ±2.5 diopters.
Why choose Trans-PRK?
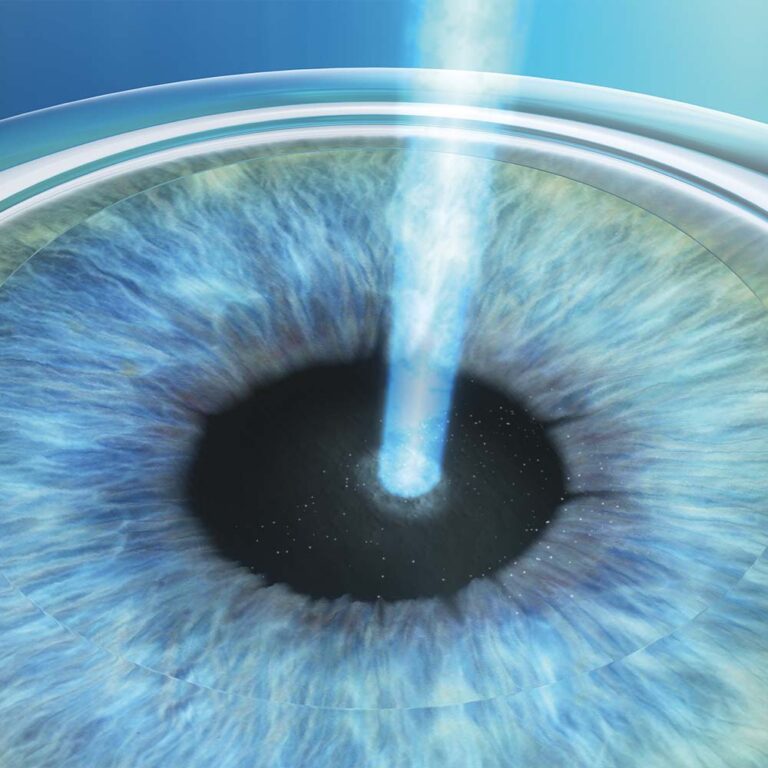
Trans-PRK is a surface procedure in which the corneal epithelium is removed non-contact using an excimer laser. The acronym Trans-PRK stands for transepithelial PRK.
Using a laser for epithelial removal ensures that the stroma is free from minor irregularities before the corrective procedure. The stromal bed is perfectly even before the vision correction process begins, maintaining uniform humidity and temperature conditions across its entire surface.
Since there is no need to create a corneal flap or use the epithelium as a “masking substance,” this method can be carefully applied to corneas with minor irregularities, as well as in selected cases of keratoconus.
Mild Nearsightedness (Mild Myopia) and Myopic Astigmatism, Mild Farsightedness (Mild Hyperopia) and Hyoperopic Astigmatism, Mild Astigmatism
Patients with shortsightedness (myopia) up to -3.5 diopters, possibly with accompanying astigmatism.
Patients with farsightedness (hyperopia) up to +2.5 diopters, possibly with accompanying astigmatism.
Patients with astigmatism up to ±2.5 diopters
Why choose Topo-guided?
Topo-guided PRK is a surface procedure in which the corneal epithelium is removed either mechanically or non-contact. If the epithelium is removed with a laser (non-contact), the method is referred to as Topo-guided Trans-PRK.
The Topo-guided PRK method has two primary goals: correcting the refractive error and smoothing significant corneal irregularities.
Topo-guided PRK is a technique where the laser program is based on the specific corneal topography. It is highly effective for severely irregular corneas, such as those after trauma, multiple surgeries, or in certain cases of keratoconus and other corneal degenerations.
Mild Nearsightedness (Mild Myopia) and Myopic Astigmatism, Mild Farsigthedness (Mild Hyoperopia) and Hyperopic Astigmatism, Mild Astigmatism
Phakic Lens Implantation (pIOL) Phakic lens implantation is performed to correct vision in patients for whom laser vision correction is either contraindicated or would not offer the expected results. The procedure involves implanting an artificial lens made of a specialized composite material called Collamer. Collamer is a combination of naturally occurring collagen, which provides high biocompatibility while maintaining durability and transparency. Phakic lenses are implanted adjacent to the patient’s natural lens. Preserving the eye’s own lens is a key advantage, as the patient’s accommodation remains unchanged after the procedure.
The Procedure The implantation is performed under local anesthesia after pupil dilation and takes approximately 30 minutes. The first step involves creating a corneal micro-incision (microport) 2–3 mm in length. A sterile gel (viscoelastic) is then injected into the eye chamber, allowing for the implantation of a folded lens without touching the eye’s internal structures—including the patient’s own lens and cornea. Once implanted, the lens begins to unfold spontaneously due to body temperature and the presence of the viscoelastic. After the lens is fully unfolded, the surgeon positions the phakic lens correctly in the posterior chamber. The corneal micro-incision seals itself and does not require sutures.
Reversibility Phakic lens implantation is a reversible procedure. In the event that a patient develops cataracts later in life, the clouded natural lens is removed along with the phakic lens. A standard intraocular lens (IOL) is then implanted to compensate for the power of both previous lenses, ensuring the patient’s visual outcome remains consistent.
High Shortsightedness (High Myopia), High Farsightedness (High Hyperopia), High Astigmatism
I had the SMILE procedure and I'm delighted. The doctor is a true professional – everything was thoroughly explained to me before the surgery, and I felt safe and at ease during the procedure. The procedure itself was quick and painless, and the results exceeded my expectations – my vision is excellent, better than ever before. Post-operative care was also top-notch; I could always count on answers to my questions and support.
I wholeheartedly recommend him to anyone considering vision correction – it was one of the best decisions of my life!
I highly recommend Dr. Marcin as a top eye surgery specialist in Warsaw. The procedure was totally painless and the service l have gotten was great. Now, l can see this World properly thanks to the Doctor. My sincere recommendation to everyone.
I had a lot of concerns about vision correction. I was afraid something would go wrong and I'd have to deal with the consequences. Ultimately, I went for a consultation with Dr. Smorawski on a recommendation, as he had performed the procedure on a family member a few years ago. And that was the moment I believed him. Dr. Smorawski is full of empathy and patience, personally greets and gets to know each patient, answers all questions honestly, is extremely knowledgeable and professional, and his personalized approach makes you feel completely cared for. This isn't a chain store where you have to wait for a hotline to be connected, so in case of an emergency, you can count on him.
Ms. Agata, who supports the doctor, also inspires great trust, offers advice, and patiently answers questions. 😉 I've been having my vision correction done for a few weeks now, from -3 to 0, and my quality of life has improved significantly. I can only say that I regret waiting so long. I would choose the same place again, and only Dr. Smorawski. I recommend it 100%.
If you are looking for an ophthalmologist I highly recommend the Smorawski Okulistyka clinic.
Dr. Marcin Smorawski performed my SMILE procedure lately, and I had the pleasure of receiving his excellent care. From the very first consultation, Dr. Smorawski impressed me with his professionalism. He patiently answered all of my questions and took the time to thoroughly explain every step of the process. His ability to make complicated medical concepts understandable gave me the confidence to feel well-informed and secure in my choice. The results of the LASIK surgery have been life-changing, and I owe it all to Dr. Smorawski’s expertise.
Laser Eye Surgery Techniques - consultation with a specialist
Are you struggling with vision problems and want to effectively eliminate them? Contact us to determine the treatment method best suited to your case.
To provide the best experiences, we use technologies like cookies to store and/or access device information. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional
Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.
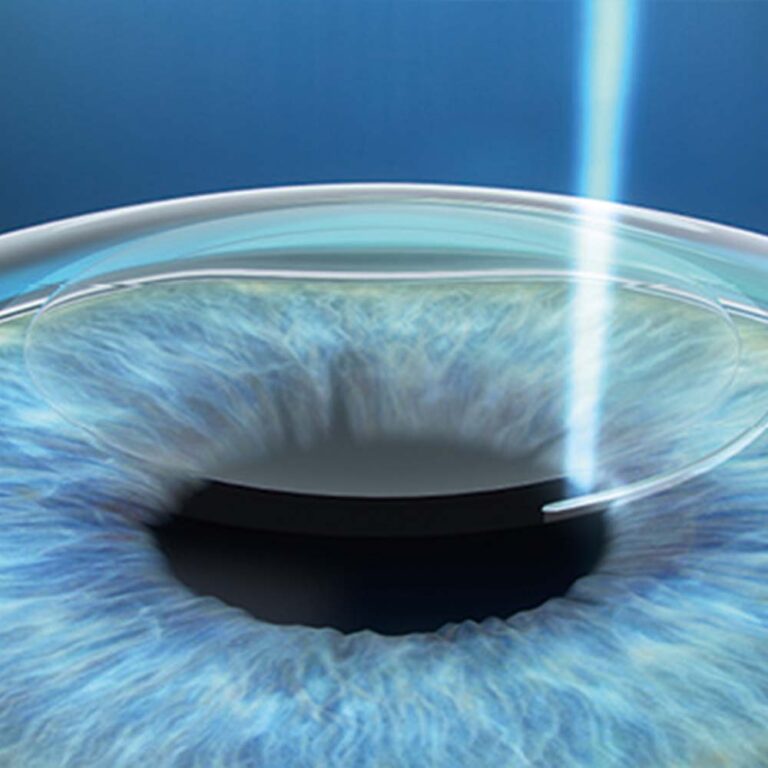
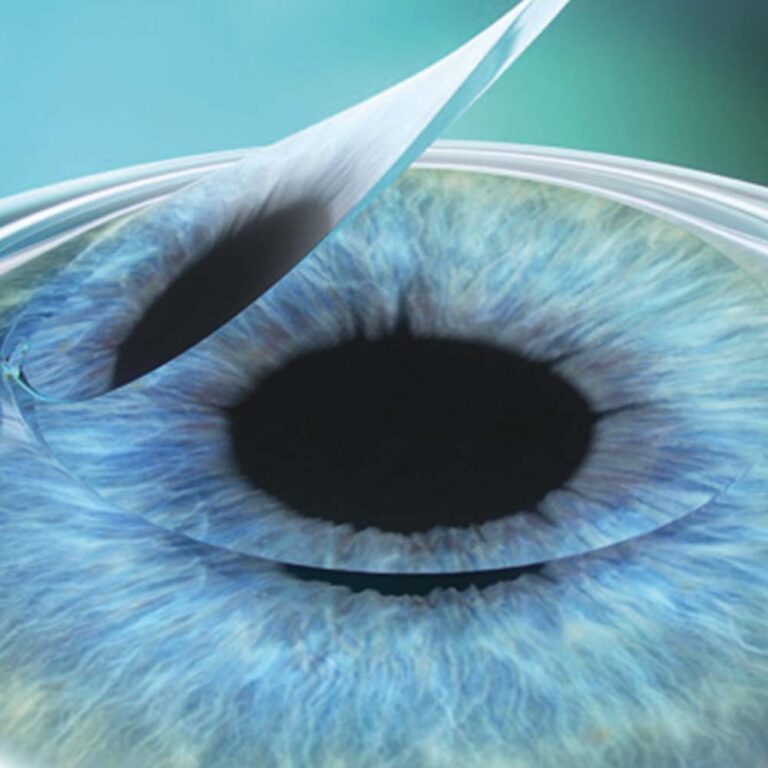
The corneal surface (the outer part) is its most valuable layer. SMILE technology leaves this vital outer section intact, as the procedure removes tissue only from the deeper layers of the cornea. As a result, corneal stability and strength after the procedure are higher than with any other method. For example, correcting 4 diopters of shortsightedness using the SMILE method leaves the cornea significantly more resilient compared to other correction techniques such as Femto-LASIK or PRK.
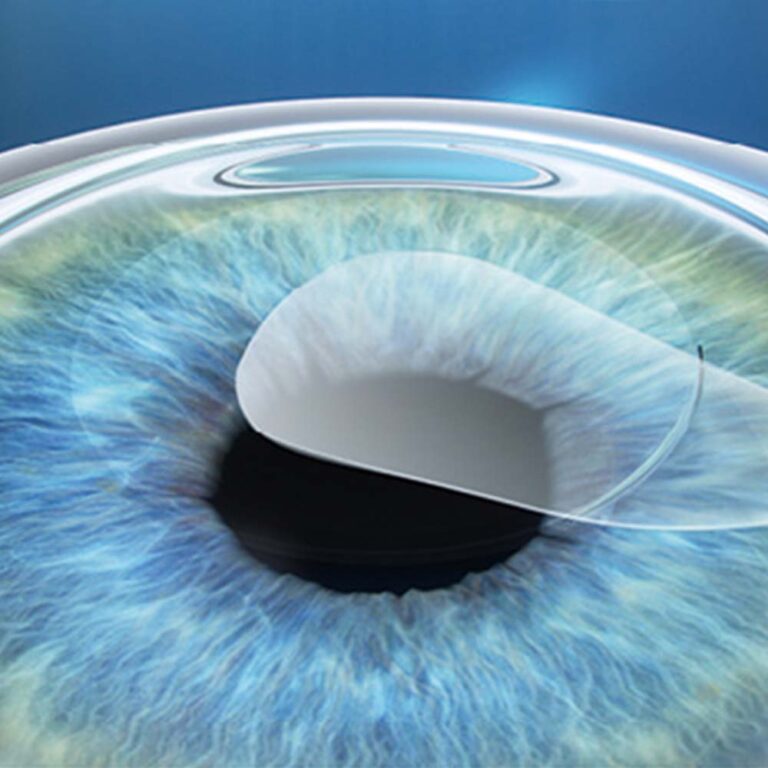
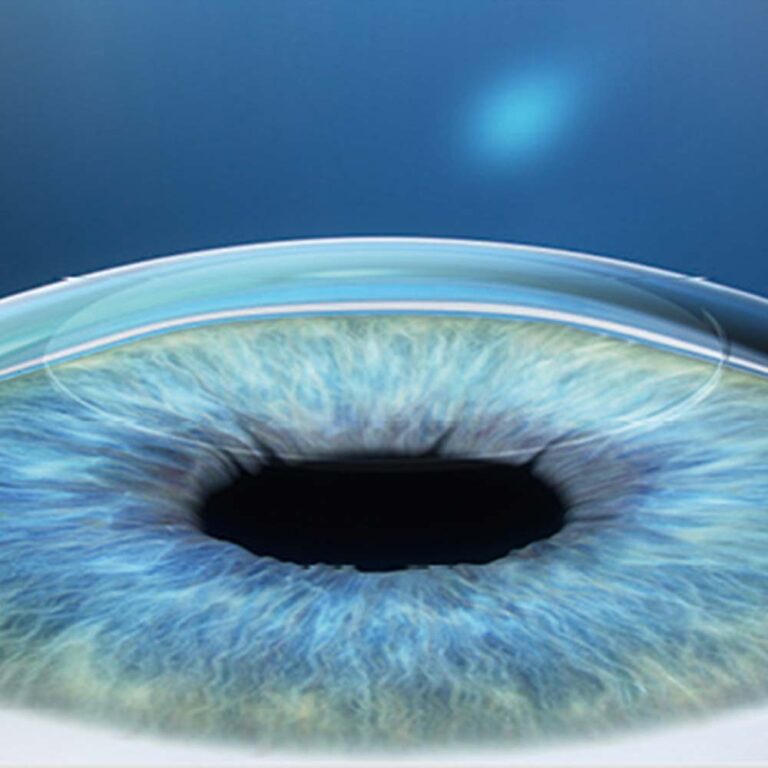
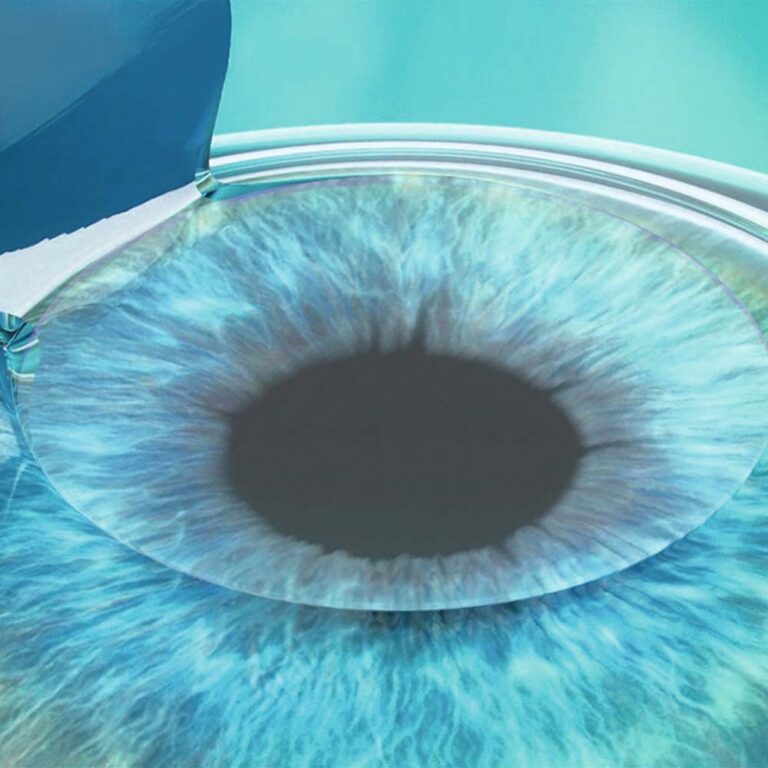
SMILE technology works by creating a thin disc of tissue (lenticule) within the deeper layers of the cornea. Once this disc is removed through a tiny micro-incision, the cornea flattens and its refractive power is reduced. This effectively eliminates shortsightedness or myopic astigmatism—the two primary vision impairments for which SMILE technology is utilized. Consequently, the procedure does not require a corneal flap.
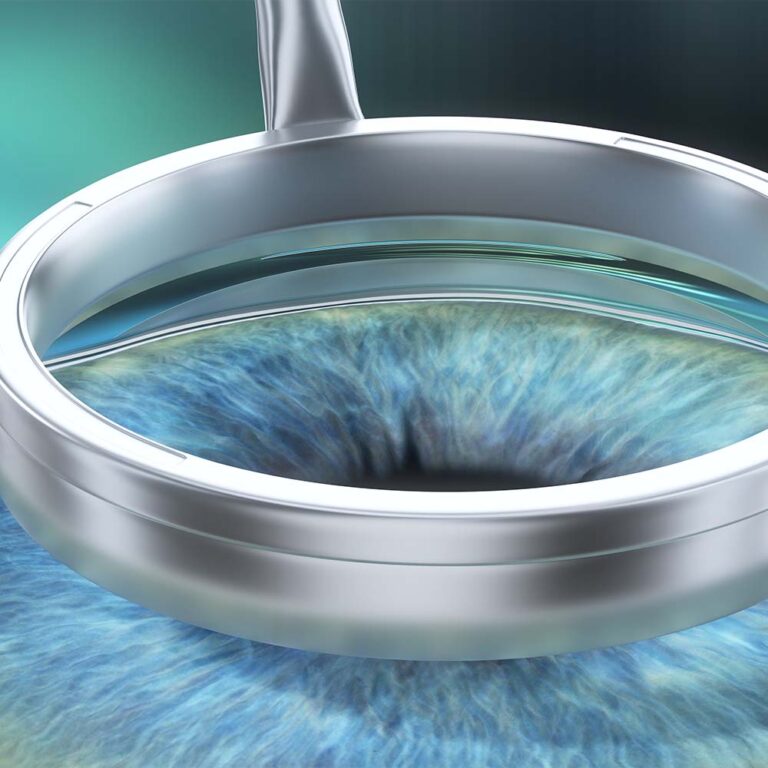
Hyperopia, hyperopic astigmatism, and astigmatism are the most resistant refractive errors to correct. To eliminate farsightedness, a change is required that results in increased corneal steepening. Steepening the corneal dome is significantly more challenging to achieve with laser correction than flattening it. This creates the need for a procedure with a higher EMO (Effective Modifying Power), which is more effective at reshaping the tissue. Femto-LASIK is such a procedure. It is a two-stage treatment. The first stage, which involves creating a corneal flap, simultaneously reduces the rigidity (softens) of the cornea. Once prepared this way, the cornea becomes much more pliable and susceptible to reshaping during the second stage. In the second stage, an excimer laser is applied to the corneal stroma exposed under the flap. In the treatment of presbyopia, we take advantage of the practicality and easy access provided by the presence of the corneal flap. As we age, the demand for visual power for near-distance work increases. To meet this growing need, we can compensate for the increasing near-vision impairment through a minimally invasive and simple method: a flap lift.
Presbyond gives the cornea a specific shape. After treatment with this method, the cornea has varying curvatures in different areas. This allows for increased corneal power in the specific zones used for reading, providing the patient with the additional boost needed for near-distance work.
However, not every patient is a candidate for the Presbyond procedure. Its effectiveness and feasibility depend on the initial corneal parameters, primarily the pre-operative corneal curvature, which is measured and evaluated at critical points.
EBK and PRK are surface vision correction methods in which the first, preparatory stage is the removal of the corneal epithelium. In PRK, the epithelium is removed manually using a special solution that loosens the connection between the epithelium and the corneal stroma. In EBK, also a manual method, a specialized device called an epikeratome is used to remove the epithelium. The corneal epithelium regenerates—or regrows—within several dozen hours, forming a perfectly smooth and even surface. The epithelium has a massive impact on visual quality, and even microscopic irregularities on its surface can drastically impair vision.
The epithelium is a fascinating structure with the ability to mask any imperfections of the underlying stroma. This characteristic is very often utilized in the treatment of corneal irregularities and keratoconus.
Why is Trans-PRK correction more predictable?
The epithelium covers the corneal stroma and is its outermost layer. In surface methods (EBK, Trans-PRK, Topo-guided-PRK), the first step is the removal of the corneal epithelium. Due to the specific way the laser operates, removing the epithelium with a laser leaves the cornea highly uniform in terms of surface texture and hydration levels. The correction stage follows immediately after the epithelial removal phase, making the overall result significantly more predictable compared to manual removal.
What does it mean that the epithelium can be used as a masking substance?
The human eye is not perfect; minor irregularities often occur on the corneal surface. These are frequently compensated for by the overlying epithelium. Thus, the epithelium acts as a tissue that masks imperfections in the corneal stroma. When removing the epithelium manually, these surface imperfections are exposed rather than eliminated. However, by using an excimer laser for epithelial removal, we eliminate corneal irregularities along with the epithelium, achieving an optically ideal surface.
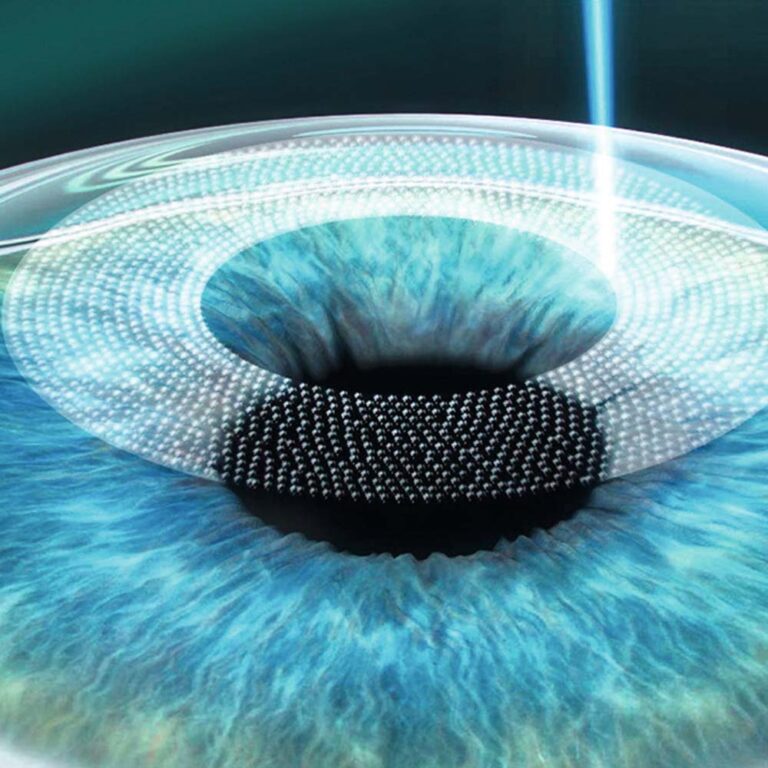
Topo-guided PRK treatment is fully integrated with corneal topography. Topography is a diagnostic test that analyzes light reflected from the cornea, sent in the form of several dozen concentric rings. Any areas of the cornea that reflect light in a distorted manner are analyzed to identify specific surface irregularities. Based on this analysis, a customized laser program is established to not only correct the refractive error but also to regularize the corneal surface in areas where it is irregular.
Phakic lenses offer the widest range of vision correction of all available methods. It is important to emphasize that they serve as both an alternative to laser vision correction and a viable treatment option for patients where laser treatment would not deliver satisfactory results. With this correction method, there is no tendency for regression (recurrence of the refractive error).